



One Big Beautiful Bill or Beautiful Nightmare "Act"?
Always looking for the silver lining

I’ve been reviewing what is now immortalized in US history as the “One Big Beautiful Bill Act” for just shy of two months now. It was first introduced on May 16th and by May 20th it was officially under review by the House Budget Committee. The day after which my own visit to Capitol Hill cooincided with President Trump’s personal visit to deliver his message “Don’t f- - - around with Medicaid”.
Fitting on two accounts.
While I was on Capitol Hill in a “standing room only” meeting to be part of a rally call for chronic disease reversal via Food Is Health and Medicine where friends like
, Pamela Schwartz and others took to the podium to deliver a message of hope, enthusiasm, realism, accountability, economic sustainability and action, Trump was on Capitol Hill behind closed doors to directly lobby with House Republicans “to personally pressure them to support his so-called One Big Beautiful Bill urging GOP holdouts to stop dragging their feet, warning them with “f-bombs” not to mess with Medicaid and even floated the possibility of primary challengers for dissenters” while also briefly meeting with Speaker Mike Johnson and Freedom Caucus members in a closed-door sessionThe juxtaposition of two seemingly divergent ideologies on the surface grounded in the same goal of reversing chronic disease for even the most economically challenged.
Fast forward 45 days to the 4th of July and the “One Big Big Beautiful Bill Act” was signed into law. Again the juxtaposition of something seen as so tragic by so many was signed into law on the day we celebrate our indepedence as a Nation is not lost.
The Controversy of Change
created some controversy this weekend when he shared a lesson learned that can easily be interpreted to imply support for the cuts in the bill, by sharing “I remain unmoved by the cuts to Medicare and renewable energy”.The controversy was a reminder that policy change is deeply personal. And that goes for every single piece of policy change. It just so happens this particular policy change effects over 80 million of the most vulnerable Americans. Four in ten U.S. children and around 15% of adults receive Medicaid or CHIP coverage. Trump may get his way most times but not this time. It seems those he met with behind closed doors on May 21st didn’t mind “F-----ing” with Medicaid despite his warning.
But here is the thing, this isn’t a policy proposal any longer, it’s now signed into law. Like it or not, we simply must move forward. It isn’t meant to be callous, it’s meant to as a call to action to forge a new path.
We are currently spending 3.5% of our GDP on healthcare for the most vulnerable, which is closing in on 25% of total healthcare costs and it’s believed up to 80% of those costs are related to chronic disease. What we are doing today is not working. Period.
Whether a chainsaw, sledgehammer or scalpel should have been used for the redesign, it’s no longer up for debate.
When you use that as the context for reading Carter’s post, it becomes a rally cry for change.
“Creative Destruction will accelerate progress faster than government funding.” perhaps adding the word “de-funding” to this sentence adds an important nuance.
He goes on to say…
“Change is essential if we want to break free from the dysfunctional capital allocation system in corporations, who prefer maintaining the status quo over investing in R&D.
The US innovation system outpaces any other globally when market forces push it to innovate. We are now at a perfect storm: engineers can leverage AI as a superpower to multiply their output tenfold.
We share a collective vision of what food can do for health and what renewables can do for energy. We have a young workforce indifferent to rigid institutional structures. The wind, tide, and talent are aligned to enable multiple market breakthroughs. Any of which will improve the human condition.
Markets don’t fail from lack of demand; they fail from poor signal integration. Hayek was right, economic resilience comes from bottom-up decision making, not top-down control.
Innovation works because it matches knowledge to action more quickly than policy ever can. We are in an innovation period akin to 1930-1960, which saw transformational breakthroughs in healthcare, energy, food, transportation, etc.”
A Rally cry. A design challenge. A vote of confidence in the private sector. A call to action. A sentinel moment. A once in a lifetime window of time. A wormhole. It’s all of these things.
The Interconnectedness of Tragedy & Opportunity
Somehow I’ve always been able to compartmentalize things by combining action and silver linings. It’s a blessing and a curse. Many times it’s misinterpreted as being callous. It’s quite the opposite, it’s my coping mechanism. Think of it as “Action after Reaction”.
The Tragedy (Reaction)
The $4.5 Trillion in Tax Cuts that make 2017 tax cuts permanent could reduce federal revenue available for everything needed in System B and some of System C including things such as public health and nutrition programs, potentially hindering efforts to prevent disease.
$1.1 - $1.3 Trillion in Medicaid cuts over 10 years - People in the lowest 10% of income distribution in the U.S. stand to lose noncash government benefits such as Medicaid coverage and food stamps worth nearly $1,600 annually on average, according to an analysis of an earlier version of the bill by the Congressional Budget Office.
Leading to a loss of health insurance coverage for up to 12 million (excluding those losing coverage due to expiration of ACA subsidies)
Medicaid work verification begins in 2027 and show that they have spent 80 hours a month working, volunteering or attending school.
Provider taxes and state-directed payments reduced starting in 2028
SNAP (Food Stamp) Cuts of up to $300 Billion Increases food insecurity, especially among children and low-income families combined with prohibition on Thrifty Food Plan (TFP) Increases - USDA barred from increasing TFP cost except for inflation adjustments, limiting SNAP benefit increases and limits on SNAP Benefit Adjustments tied only to CPI, not actual food costs or nutrition needs
Cuts to Social Welfare Programs Beyond SNAP/Medicaid - reductions in other safety net programs, potentially including school meals or WIC
Medicaid Provider Tax Reductions will cap and reduce provider taxes that states use to leverage federal Medicaid funding - referred to below as “state-directed payments”. Currently, taxes are capped at 6% of healthcare providers’ net patient revenue, but will be reduced to 3.5% in expansion states. In non-expansion states such as Florida and Texas, tax rates will be frozen in place up to the 6% maximum as of July 4th 2025. The taxes have been criticized as a gimmick and even Obama tried to cut them. Some states such as NC have used the taxes to fund their Medicaid expansions. According to one firm, the most significant reductions include MT 21%, AZ, KY and VA 18% each, CA13% and NY 9%
Introduction of copays for treatments such as dialysis, potentially costing patients thousands annually
ACA (Obamacare) Marketplace Cuts of $268 billion from ACA marketplace due to subsidy expiration combined with elimination of automatic ACA reenrollment, increasing uninsured rates by as many as 5.1 million by 2034
$500 billion in cuts 2026 - 2033 in Medicare cuts via the Statutory Pay-As-You-Go (S‑PAYGO) law which triggers sequestration - administered automatically, these payment cuts will mainly impact provider/facility revenue
The $500 million MAHA (Make America Health Again) initiative did not survive enactment in the final One Big Beautiful Bill Act. The discretionary funding line was dropped during reconciliation. MAHA funding will need to be reintroduced and funded through future appropriations bills (annual federal budget legislation).
How the Tragedy Unfolds aka Rolls Downhill
Let’s start with the healthcare industry (aka Deathstar). It’s important to begin by understanding the true magnitude of the healthcare industry to our economy.
Assuming healthcare takes the most direct hit from the Medicaid and Medicare cuts, the knee jerk reaction is to think healthcare is the only one in for a world of hurt. When you look at the graphs below from a recent NYT article, healthcare is literally the top employer in over 75% of states. Let that sink in for a second. To say that we have monetized sickness is an understatement.

Here is the kicker, it’s not what you think.
Much like my lifespan epiphany in May, the devil is in the details.
Large employers are in for what could be a potentially equal world of hurt. But first let’s start with hospitals and watch it roll downhill.

It’s important to note when looking at the graph above that the healthcare economy isn’t built upon the Medicaid population and Medicaid revenue. In fact the reimbursement rates are notoriously low. Instead it is built upon the TOTAL healthcare spend, of which big volume comes from Medicare but which margins are funded largely by the commercial segment aka large employers.
There is not one hospital in the country that can stay in business with only Medicaid (I’m excluding the most rural of the rural that have managed to keep the lights on as well as all-payor states such as Maryland). In general, hospitals can only stay in business if they have the right amount of commercial volume to subsidize/offset the Medicaid segment and to a lesser extent the Medicare segment. Of course this has blurred a bit with “state-directed payments” which artificially raise the Medicaid payment rates. 30 states will likely see reductions in these state-directed payments according to an analysis by KFF.
Most hospitals are not what is called “Medicare break-even”, so although Medicare “volume” is vital, when combined with Medicaid, government programs typically generate a “loss”. To add further perspective, Medicaid reimbursement is often at least 20% less than Medicare reimbursement. The only thing worse than having a high % of Medicaid beneficiaries in your mix of business? Uncompensated care aka uninsured patients.
So what happens when a sizeable chunk of the Medicaid segment loses health insurance? You guessed it - it becomes uncompensated care.
There is this fun thing called the Emergency Medical Treatment and Labor Act (EMTALA) which requires any hospital with an emergency department that accepts Medicare (which is most U.S. hospitals) to provide a medical screening exam to anyone seeking emergency care, regardless of insurance status or ability to pay. If the person is found to have an emergency medical condition, they must stabilize the person before discharging you or transferring to another facility. Care cannot be delayed or denied to ask about insurance, payment, or citizenship status during the emergency evaluation and stabilization.
Let’s go back to the tragedy summary above. It is estimated that the Big Beautiful Bill Act will result in up to 7-12 million (10-15%) of the 80 million people currently covered by Medicaid losing coverage by 2034. In 2023, 1 in 4 hospital days were paid by Medicaid which means up to 4% of hospital days currently reimbursed will shift to being uncompensated care.
One quantitative analysis of the compounded effect of the Medicaid cuts above calculated over the next decade that payments to hospitals will be reduced by ~$665 billion, while uncompensated care costs will increase by over $80 billion over the same period of time, according to an analysis of the bill by America’s Essential Hospitals.
Now think about healthcare access when you are uninsured, you are only guaranteed treatment when it’s emergent. So those without insurance or access (rural areas) regularly delay preventative care which generally leads to higher acute care consumption further down the line.
What most are not talking about is that hospitals’ first line of attack for this increase in uncompensated care and lower Medicare reimbursement rates will be to pass that cost on to employers in the form of higher unit costs aka reimbursement rates. Those costs subsequently get passed along to employees via a combination of higher health insurance cost sharing, benefit reductions, less choice of clinicans/facilties (aka narrow network) and/or higher deductibles/coinsurance/copays.
What happens to cover the remainder of lost revenue not subsidized by other segments?
Hospitals begin “rightsizing”. We will see more and more health systems such as Providence, one of the country’s largest health systems, who last month that it had implemented a restructuring plan that would lead to 600 employees losing their jobs
Health systems and providers halting construction for facility expansions
Investments in advanced treatment/technology dry up
The end of earnings of for-profit health systems who have doubled-down in monetization of sickcare through traditional fee-for-service reimbursement while leveraging state-directed payments - like HCA and Tenet
Closures of hospitals who don’t have the luxury of cross-subsidization such as safety-net hospitals
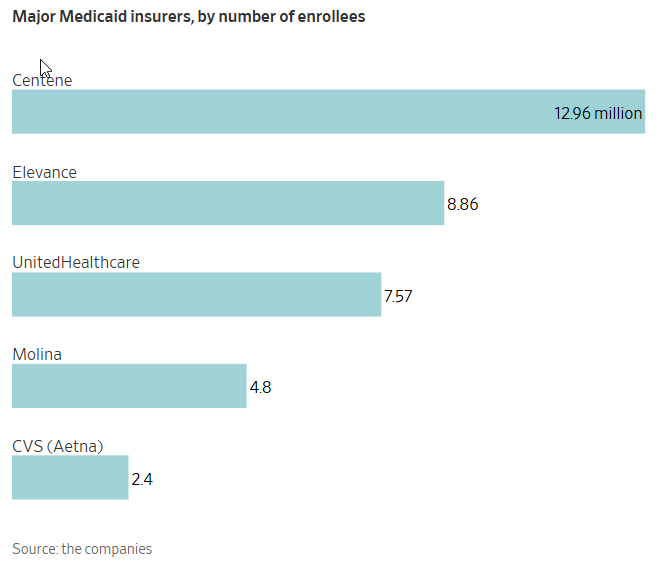
Insurers lose billions in Medicaid AND ACA (“Commercial”) revenue as eligibility and/or subsidies end for large numbers of members - case in point - Centene already withdrew it’s 2025 earnings last week
The dreaded “deathspiral” for insurers in the ACA segment when subsidies dry up for enrollees - the sickest stay and the healthiest leave - premiums can’t keep up with exponentially rising costs of the remaining insured
The Opportunity (Action)
We have two paths forward here…
Focus on the tragedy
Look for the silver lining aka opportunity
We have chosen in this substack to always focus on systemic redesign, long before the Big Beautiful Bill Act was even conceived. Even before the Make America Healthy Again (MAHA) term was coined. Everyone that reads this substack knows a complete overhaul and redesign is needed with or without policy.
Like it or not, we have a new law. Starting today, we will focus little on the details of the bill and instead focus on finding the opportunities created from the new law.
Bottom line - healthcare is losing 20% of it’s revenue stream. A revenue stream built upon chronic disease. Yet, the chronic disease itself will remain.
Let’s reframe the lens. Instead of focusing on redesigning healthcare, we now have to solve for chronic disease “without” healthcare.
The graph below helps with the reframing from an economic perpsective.

Since 1929 the interrelationship between food and healthcare appears undeniable.
Healthcare as a percent of household spending has exponentially increased, especially in the last 40 years
Meanwhile the combined cost of healthcare and food has remained a constant ratio of household spending, despite healthcare and food costs changing dramatically over the same period
Now let’s jump back into Carter’s lessons learned. That show they weren’t meant to dismiss the gravity of the Medicaid cuts but instead were meant to solve the newly created design challenge of reversing chronic disease outside of healthcare for those most economically disadvantaged:
To build a person’s N of 1 digital twin - I think it’s reasonably possible to reverse engineer the nutrients consumed by a human if you know their store purchases, CGM trace, bowel movements, physical movements, and a few other casually observable factors.
The business model for Food is Medicine digital health companies might be SaaS-like and profitable if they focus on 1) lowering the cost of customer acquisition for groceries and 2) being paid for outcomes.
There is a market for a risk capital stack to support outcomes-based digital health companies. This would underwrite the transition away from the $1.9T we spend on healthcare costs of poor nutrition.
Further reframing, we can begin to see opportunities such as these:
The cuts could perhaps fuel venture investments in things such as:
Private solutions in nutrition and preventive health
Services that lower out-of-pocket costs or improve access for the uninsured could see increased demand
Direct-to-consumer to target pre-chronic
Platforms to help Medicaid enrollees track and report work requirements, or connect to qualifying activities.
Tech-enabled food banks, meal delivery, or nutrition support for food-insecure populations.
Affordable direct-to-consumer preventive care especially in rural areas
Telehealth, remote nutrition counseling, and rural provider collaboration platforms
Budgeting and meal planning apps tailored to fixed SNAP benefit levels
Rural health system efficiency tools, alternative care delivery models
Payment assistance platforms, or bundled care models that reduce patient costs
Enrollment support and navigation services
Payroll and benefits platforms for small businesses
Platforms for managing and optimizing CHOICE Arrangements
Collaboration with NIH/FDA on research or commercialization of research findings
School-based nutrition programs, partnerships with local producers.
And finally the “new funding” in the new law that have been overshadowed by the cuts (tragedy):
$50 Billion Rural Health Transformation Program to create a fund for states to improve rural health access, promote technology, and prevent chronic disease
Pre-Tax Premiums for Exchange Plans that allows pre-tax payments for individual health insurance premiums on the Exchange
CHOICE Arrangements (Rebranded ICHRAs) which expands personalized health reimbursement arrangements, with tax credits for small employers
FDA-NIH Nutrition Regulatory Science Program - a new initiative to research root causes of diet-related chronic disease and inform policy
At the end of the day I can’t seem to get the image of the phoenix rising from the ashes out of my mind. Or less mythically speaking - the silver lining.
Otherwise, I’m just giving up and that just isn’t in my nature.
Medicare cuts are coming, too.
https://musingsofanobody.substack.com/p/are-we-on-a-death-watch-medicare
On the latter, don’t.
On the former, our best shot is to keep unraveling this tightly woven hairball until the strings are loose enough to start braiding a new preventive care system from the bottom up.
Prioritize. Deputize. Act.