



The Food Is Health RFI Response
Submitted in Response to the "Ensuring Lawful Regulation and Unleashing Innovation To Make America Healthy Again" Request for Information

We successfully submitted three separate RFI responses before the clock struck midnight which just so happens to coincide with my father’s 80th birthday - “Happy Birthday Papa.” If you haven’t guessed he’s a loyal (and biased) reader.
We submmitted the specific RFIs we shared in draft form last week dedicated to Modernizing Food-Health Regulations to Enable Evidence-Based Chronic Disease Claims and Enabling Innovation in Chronic Disease Prevention & Reversal but made a “game-day” decision to crate a third response.
One designed to speak to a new regulatory framework that could move beyond treating chronic disease but actually reverse it and prevent it. Effectively eradicating the current chronic disease epidemic. However, it requires a herculean coordinated effort amongst massive industries that represent over $10 trillion which represents a third of our GDP.
We convened this Food Is Health group and now movement in hopes of restoring human health along with our soil. It felt remiss not to swing for the fence and articulate a regulatory framework capable of capturing the essence and magnitude. And so, we created an overarching Food Is Health response. We thought it fitting to share the full response with our Food Is Health community and substack readers.
The Food Is Health Response
Thank you for the opportunity to comment on the Department’s Request for Information, “Ensuring Lawful Regulation and Unleashing Innovation to Make America Healthy Again.” We are writing to respond under the “Food is Health” banner, which represents a collective of thousands of multi-sector industry leaders that have convened to address human health.
The reality is that healthcare alone cannot Make America Healthy Again. Below we are outlining a vision rooted in the reversal of the chronic disease epidemic which currently accounts for roughly 90% of our nation’s $4.9 trillion annual health expenditure (as of 2023) and in preventing future avoidable chronic disease. This calls for a systemic design that aligns soil, agriculture, food and healthcare with a unified objective of human health through policy and innovation. This is how we will Make America Health Again AND ensure health going forward.
Background - The Shift to Cheap Calories and Healthcare
The 20th century unintentionally set the course of our chronic disease epidemic through a handful of events that charted our course.
The 19th century was rooted in labor-intensive occupations, lack of modern conveniences, daily routines that encourage/required movement and centered around community, recreation and active leisure.
The 20th century marked a complete shift with the mass adoption of automobiles, mechanization/automation of labor and household chores, desk-based office work, passive entertainment (television, radio, later computers and smartphones, creation of convenient food and cheap calories.
A primary driver of chronic disease which costs us >$4 trillion annually is poor nutrition and lifestyle. Americans spend about $1.7 trillion on food each year, yet an estimated $1.9 trillion in yearly healthcare costs are attributable to diet-related chronic illnesses (some estimates are double that figure). In effect, we pay twice – once for food that makes us sick, and again for the medical treatment of those sicknesses. This status quo is economically unsustainable and indicates a profound misalignment in our health system’s incentives. We treat food and healthcare as separate spheres when they are in fact deeply interconnected parts of a single value chain.
The Shift from Inherent Health to Cheap Calories and Convenience
At the turn of the century, food was whole, minimally processed and primarily seasonal, often local. Traditional preservation methods such as drying, curing, canning and fermenting were used for shelf-stability and seasonality. There were limited additives and preservatives, diets were regional and seasonal and home cooking w/communal eating was the norm.
The Green Revolution was established to eliminate famine looking at the convergence of environment, population and food security, it’s success led to new crops that in some cases tripled production and all but eradicated famine.
Mechanization of agriculture to improve yields and reduce cost led to tractors, combines, and other machinery greatly reduced human labor needs with the share of U.S. workers in agriculture falling from 41% to 2% while U.S. farm production more than doubled for less than a third of the labor cost while average farm size almost doubled from ~215 acres in 1950 to 487 acres by 1997; meanwhile soil organic matter declined by 50%, nutrient density declined markedly (e.g. calcium in broccoli 50% lower) and 2 tons of topsoil per acre are lost annually while chemical load skyrocketed (fertilizer 50% and pesticide almost 150% on major crops).

Food Science & Marketing became engines to capitalize on mass-production and cheap calories focused on convenience and not nutrient density. During the last half of the 20th century the food manufacturing and retail industry value grew from $300 billion in the US to $3.6 trillion in the global processed and packaged food segment alone. Food science led to the development of foods designed to achieve the “bliss point” and “mouth feel” creating the greatest craving, “sensory-specific satiety” to override the brain’s signal to stop eating and ultimately the bliss point curve to maximize bliss and profit. Marketing tactics tapped into the limbic brains love of sugar, fat and salt, focusing on young, poor and vulnerable populations designed to drive sales/profitability and not health with claims they are not responsible for consumer preference but simply respond to demand.
The Shift from Inherent Health to Healthcare
At the turn of the century, healthcare was sought for acute sickness and injury. It was delivered locally, paid directly at time of service many times through bartering of crops, livestock or manual labor. Healthcare was a personal, relationship-based service delivered primarily in homes, small clinics, or charitable hospitals.
Flexner Report sets the course for high cost healthcare. It was responsible for a wholesale redesign of healthcare delivery from community-based to university-affiliated hospitals by radically reforming medical education, leading to the catalyzation of a model integrating medical schools with hospitals, prompting a shift requiring scientific, research-based medicine spurring biomedical research investments, flipping hospitals from charity to prestige, leading to the closure of many medical schools especially Black and Women’s medical schools and physicians and limiting/eliminating rural healthcare.
Prepaid hospital expense plans offered by Baylor Hospital covered up to 21 days and shifts to insurance plans when Blue Shield is formed that begins to include physician fees, blurring the lines of health insurance and providing healthcare coverage.
IRS Ruling exempts employer-based healthcare from taxable income, incentivizing employer-sponsored coverage inadvertently separating employees from their healthcare coverage - employers handle benefit design and cost transparency is eliminated.
Mass adoption of vaccines and antibiotics leads to exponential improvements in child mortality and premature death rates and increasing overall life expectancy.
Creation of Medicare and Medicaid to cover healthcare costs of seniors, low-income and vulnerable population leads to the coverage of diagnosing and treating healthcare conditions, not prevention, inadvertently incentivizing ongoing diagnosis and treatment.
Current Procedural Terminology (CPT) codes established as a standardized system of terms and codes to describe medical, surgical and diagnostic services for the purposes of documentation, reporting, and billing leads to the fee-for-service payment system.
Employee Retirement Income Security Act (ERISA) created to govern employee health benefit plans amended by COBRA, HIPAA and ACA eliminates benefit design innovation.
Health Maintenance Organization (HMO) Act backfires due to economic misalignment using physicians as gatekeepers instead, using denials, paying capitation and withholding care instead of addressing root cause and preventing disease as intended.
Preferred Provider Organization plans replace indemnity insurance plans and use reimbursement rate negotiations to lower costs as opposed to reversing disease.
Omnibus Budget Reconciliation Act of 1989 (OBRA 89) mandates the creation of a standardized, resource-based (productivity) schedule for physician services which led to the Medicare Physician Fee Schedule (MPFS) using the Resource-Based Relative Value Scale (RBRVS) to assign relative value units (RVUs) based on physician work, practice expenses and professional liability insurance costs and adjusted geographically to determine Medicare payments which led to what services were covered and not covered and a productivity based focus leading to more patients seen and less time with patients.
Medicare introduces the Prospective Payment System (PPS) and Diagnosis-Related Groups (DRGs) for hospitals - the faster the discharge the higher the margin.
The Impact on Human Health
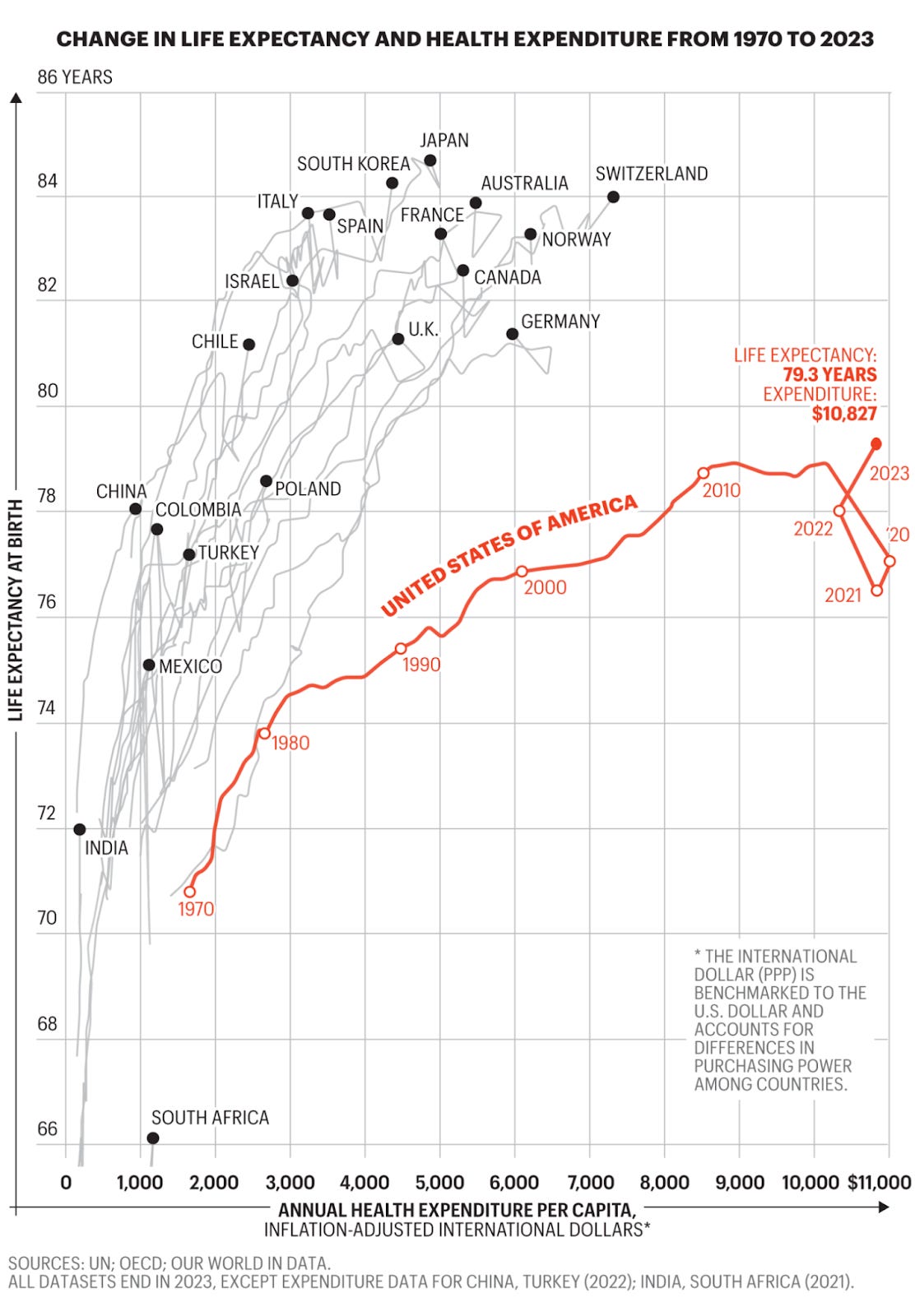
Many falsely attribute what we know as modern medicine in the 20th century with an increase in life expectancy of 30 years. While statistically accurate, the wrong conclusion is drawn. When death prior to age 20 is removed from average life expectancy from the 1800s, average life expectancy was typically 60-65 years. Vaccines and antibiotics added another 5 years to 71 in the 40’s and 50’s. Since that point, we have gained a final ~7 years of life expectancy at the cost of $2.1 trillion in annual healthcare cost ($6k per capita). Meanwhile our life expectancy improvement overlaid with cost compared globally demonstrates failure.
While modern medicine advancements have accelerated at unprecedented rates, so has the rate of chronic disease, particularly avoidable/reversible disease. Metabolic dysfunction contributes to up to 75% of all chronic disease. Less than 7% of the US population is considered metabolically healthy.
To reverse this, the answers are not found in reforming the existing healthcare system, but in our soil, on our farms, in our grocery stores and restaurants and in our homes. The pillars of lifestyle lead to metabolic health and the eradication of upwards of 75% of chronic disease.
A New Regulatory Approach - Human Health
When we consider Making America Health Again, we tend to focus on the $4.9 trillion dollar healthcare industry as the answer, half of which is funded by the government for Medicaid and Medicare. However, as we outlined above, the healthcare industry was created to treat sickness and keep people alive as long as possible not to prevent disease or reverse it.
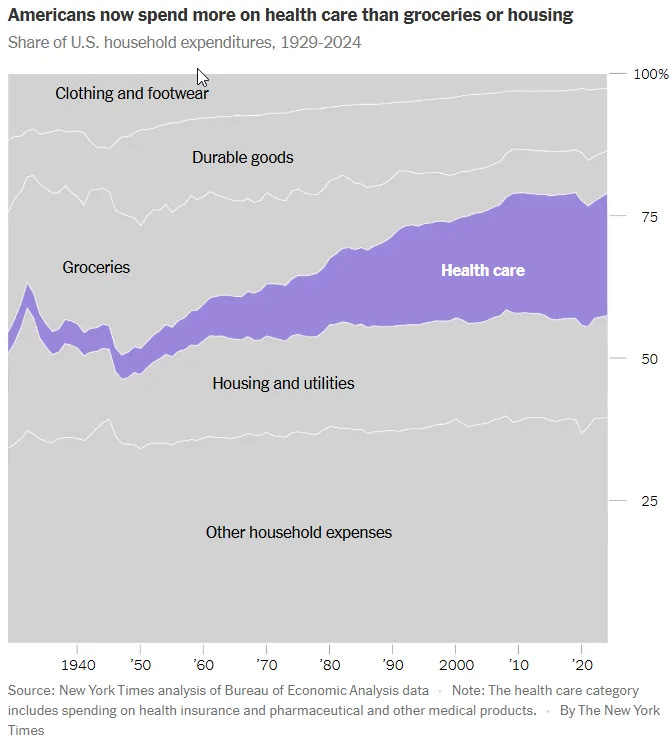
Interestingly enough, even household expenditure data shows the interrelationship between groceries and healthcare. As calories became cheap and grocery expenditures became a fraction of annual household expenditures, healthcare accelerated with the combined cost of both remaining steady as a share of expenditures over time.
Instead, if we focus on human health, we must also consider the primary inputs. Let’s use the evidence-based six pillars of Lifestyle Medicine - Nutrition, Exercise, Sleep, Stress, Substance Abuse, Relationships. The combined economy grows to include $2.5 trillion spent annually on food (grocery, retail food, restaurants, fast food and takeout) and $1.6 trillion annually on Wellness (physical activity, weight loss/nutrition, mental wellness/stress management, personal care & beauty, wellness tourism, TCM, wellness, spas, workplace wellness and more) outside of healthcare costs. The combined economy of human health is closer to $10 trillion annually. Chronic disease is fundamentally based on prevention and we’ve misallocated the funds that determine human health.
Segmenting the Human Health Economy not the Healthcare Economy
This is a segmentation that could be used as the framework for a new regulatory approach to address human health with the objective to reverse and prevent the 75% of chronic disease that is a result of metabolic health while improving effectiveness for the treatment of the remaining 25% of healthcare cost.
It is easiest to start by using the current healthcare expenditures risk pyramid (the figures below are illustrative and vary by cohort) used within the current healthcare economy:
High Cost - 10% of population, 50% of the cost (includes multiple chronic conditions, frail, elderly, genetic disorders, complications, catastrophic injuries/illnesses) - we currently view this category as unlikely to move back into one of the lower-need categories because we do not have an established disease reversal track/option, as that is misaligned with the economic model designed to reimburse for ongoing treatment.
Medium Cost/Rising Risk - 40% of the population, 40% of the cost (includes those with one or more chronic condition, issues with medication adherence, above average utilization) - this group will move into the high cost group without lifestyle interventions but today those interventions are not offered and/or sufficiently reimbursed in lieu of ongoing treatment for what has already been diagnosed.
Low Risk - 50% of the population, less than 10% of the cost (includes those at marginal risk, stable and healthy) - the majority of this group will move into the medium risk category without lifestyle medicine/support (with a heavier weight on nutrition) which is not offered through healthcare but via employer wellness and discretionary spending.
As of today, the healthcare industry is designed to monetize illness. Therefore the focus is almost exclusively on the high cost segment of the population along with those in the medium risk segment utilizing healthcare. As of today, the 75% of chronic disease behind that cost burden that is reversible is merely treated and managed. There is no established disease reversal track/option. By monetizing treatment, a faulty economy has become entrenched that fails to recognize that motivations vary not by cost tier but by priority.
We propose a new regulatory framework that focuses on human health and ends the chronic disease epidemic by simultaneously stopping the flow of chronic disease, reversing chronic disease and preventing disease by rebuilding health from the foundation.
#1 - Support of Health - Prevent Disease
There is no economy focused on this objective today. Yet it represents the future pipeline of chronic disease and healthcare costs. Stop the pipeline, stop the chronic disease epidemic. We consider this the “Pre-chronic market” made up of as many as 170 million Americans. This segment is currently undefined and is largely ignored by the healthcare industry. It represents ~3% of healthcare costs within the healthcare industry. Yet we know that >93% of Americans are at risk for metabolic disease due to factors such as poor diet and weight gain. The flaw in the current prevention business model is that it fails to include the solutions. What we need is a prevention economy that is built upon business systems, supply chains and service offerings that centers on affordable nutrition and not cheap calories.
What we ignore is that the primary input for metabolic health, the primary driver for chronic disease, is nutrition. Therefore, our food industry is in fact responsible for chronic disease prevention (and in large part chronic disease reversal) not healthcare as it is designed. Our food industry does not yet see this opportunity but it is a critical player in disease prevention. Without the root of prevention included in the framework and economic model, prevention will not be achieved and the pipeline of disease will continue. The foundation of prevention is food for metabolic health, immune function, and cognitive performance.
This leads to innovation in agriculture and food production aimed at maximizing human health outcomes. This involves treating the food system as part of our health system. Emerging agtech companies are focusing on soil health, crop genetics, and nutrient density, asking not just “how can we grow more?” but “how can we grow more nutritious food?” Companies like Miraterra and Holganix are working on optimizing the soil microbiome and natural inputs to improve both crop yield and the nutritional profile of those crops. Others like Edacious are developing ways to measure and benchmark the nutrient density of foods and under different farming methods. Technologies to preserve nutrient content post-harvest are coming online. This “soil-rooted” innovation is creating a future where food and medicine converge at the most fundamental level to support human health.
Meanwhile a new generation of direct-to-consumer health platforms leveraging AI-driven infrastructure like Hims & Hers, Ro, Oura/WHOOP wearables, Prenuvo scans, Function Health, and even Apple are monetizing knowledge for consumers in this segment that have sufficient discretionary income. They track biomarkers, improve lifestyles, and address risks proactively. They build ongoing relationships and healthy habits long before a person would show up in a hospital . Instead of episodic 15-minute doctor visits separated by months of silence, we move care of human health into the fabric of daily life.
A redesigned food supply offering affordable nutrition combined with personalized health support on a continuous basis enables a shift from reactive care to proactive “health maintenance”, addressing issues before they escalate. The potential benefits are twofold: patients stay healthier with less need for intensive interventions, and providers are freed from some burdens (since algorithms can handle routine monitoring and nudging, clinicians can focus on complex cases). The $4 trillion chronic disease market pipeline dries up.
#2 - Restoration of Health - Reverse Disease
This is not a current pathway that exists within the healthcare or food industries. It is one that is designed to reverse disease, not treat it. This is a priority when focusing on the exponentially increasing $4 trillion of the current healthcare spend attributed to chronic disease. Reversal can be achieved through a combination of metabolic reprogramming via a combination of tools underneath the umbrella of a lifestyle focused clinical approach. It cannot however be achieved by point solutions that are not connected to the root cause. Providing access to wearables does not work without the lifestyle modification support and affordable nutrition necessary to reverse disease.
Lifestyle Medicine is the scalable clinical pathway for oversight. The evidence-based, established board certification and training is a tool that can be deployed from physicians to mid-levels to Nurses to Dieticians to Pharmacists to Dentists and even culinary specialists along with the deployment of Lifestyle Medicine Coaches. These clinicians can deploy tools such as GLP-1s which have shown dramatic drops in inpatient hospitalizations and lower total medical expenditures, Food-Based Disease Reversal / Food Is Medicine which have led to equally impressive drops in hospital admissions and reductions in total medical expenditures. These interventions can be supported by Intensive Therapeutic Lifestyle Change programs and a multitude of digital tools combining human and AI interactions along with advanced behavioral science to modify behaviors permanently. Ultimately reversing disease.
Today these options are commonly not covered by health insurance and therefore not reimbursed. As a result, consumers stick with disease treatment which is covered / paid for. Making it effectively cheaper to the consumer to be chronically ill while being detrimental to the economy and national security.
It is imperative we create an economic pathway for disease reversal to be a parallel option to disease treatment for those with chronic disease, regardless of coverage.
#3 - Treatment of Disease - Disease Management
There is little that can be done for the costliest patients when the focus is treatment. This has been demonstrated time and again over the past 50+ years. If you don’t address the root cause and eliminate or markedly improve the health status of the patient, costs remain within a 5-10% corridor despite efforts to date that have included narrow networks, HMOs, ACOs, bundles, episodes of care and value-based care. Instead, the models of excellence we tend to cite are vertically integrated models such as Kaiser that are incented to address the health of the population and not simply treat disease.
This segment will continue and remain focused on delivering acute care. However, it will rapidly retract as disease is reversed and prevented in the other domains of the framework. Note that we have submitted separate responses for both healthcare and food that focus on the key points of friction within each respective industry.
The Opportunity Beyond A New Regulatory Framework
The encouraging news is that a wave of innovation has already been funded in agriculture, food and healthcare that supports this framework but the results have been mediocre. Great strides have been made via agriculture technology, food innovation, lifestyle medicine, Artificial Intelligence and digital tools. But the friction and barriers must be removed:
Economic misalignment between food and human health with a focus on cheap calories.
A healthcare economy built solely to serve the sick and chronic and improve life expectancy at any cost.
Wellness and prevention only accessible through discretionary income most don’t have and are not linked with addressing the root cause.
Consumers that lack the knowledge and access needed to make good decisions.
Together, this new regulatory framework promises to “Make America Healthy Again” by drastically cutting the prevalence and severity of chronic illnesses. The role of government here is to enable and accelerate this transformation by removing unnecessary barriers. Our legacy regulatory frameworks, built in an earlier era of healthcare, too often hold back these new solutions. By updating regulations to reflect modern capabilities, HHS can unleash innovation and allow market forces to drive better health outcomes at lower cost.
Foster safe but rapid deployment of digital health tools. We should ensure that privacy rules, FDA device approvals, and reimbursement policies all encourage (and do not inadvertently block) the use of AI and remote monitoring in preventive care. Modernize the regulatory pathway for software-driven health innovations to accelerate their time-to-market and ongoing improvement. Expand on risk-based regulatory approaches for digital health exempting or exercising enforcement discretion for low-risk wellness software.
Create an agile review framework for higher-risk AI tools – for instance, allowing developers to make routine algorithm improvements and update their software without a completely new approval each time, as long as they operate within agreed performance bounds. The Department should build on pilot initiatives like the FDA’s Digital Health Pre-Cert program and work to implement clear guidance on adaptive machine learning in medical devices
Consider safe harbor policies for the use of AI in clinical settings: e.g., clarifying that a physician using an AI decision-support tool in good faith is not violating standard of care
Coordinate HHS nutrition efforts with USDA agricultural policy, encouraging research, and updating nutrition guidelines to reflect the importance of food quality.
Subsidization should shift to nutrient density and chemical load instead of yield.
The same way mental health and maternity became a requirement, so should chronic disease reversal centered around lifestyle.
Health insurance is allowed to become focused on catastrophic care to allow for reallocation towards lifestyle support and health leveraging HSAs and supplemental policies.
A new coverage pathway for chronic disease reversal is established within healthcare.
Public health campaigns centered on lifestyle and nutrition.
Food science and food marketing is scrutinized like other risky substances, warning labels considered for certain foods.
HHS (in coordination with FDA and CMS) should re-examine requirements for diagnostic tests and health monitoring devices requiring physician’s prescription or clinic visit even when used for wellness purposes and expand avenues for direct-to-consumer preventive testing to remove “gatekeeping” barriers for preventive self-care.
Enabling alternative access points such as retail clinics, telehealth, or at-home services and not requiring a doctor’s order for every preventive check, engaging the population earlier while maintaining quality and informed-consent safeguards. This deregulatory step would significantly augment early detection of issues and reduce the load of undiagnosed conditions that later become expensive chronic diseases.
Permanently adopt the beneficial regulatory flexibilities that were tested during the COVID-19 pandemic regarding telehealth and direct-to-consumer care delivery including geographic restrictions, originating site requirements, cross-state licensure barriers in federal programs, etc.
Working with states on licensure compacts to facilitate interstate telehealth in the private sector to enable direct-to-consumer health companies to operate nationwide, bringing preventive services to any American with an internet connection.
Identify any remaining regulatory or reimbursement policies that unnecessarily favor in-person visits over telehealth and eliminate them, so long as quality of care is maintained.
Encourage new care delivery models such as mobile health clinics, home-based diagnostics, and virtual primary care by updating regulations that currently assume brick-and-mortar, physician-centric care.
Leverage FDA’s authority to reform food labeling, standards, and claims in order to drive both industry and consumers toward nutrient-dense, health-promoting foods.
Prioritize, finalize and implement enhancements to nutrition labeling that emphasize nutrient density and overall health value of foods. (e.g. front-of-package labeling offering at-a-glance indicators)
Swiftly update the definition of the term “healthy” on food packaging to align with current nutrition science, thereby allowing truly healthy foods (like nuts, seeds, high-fiber foods) to bear the claim and disallowing foods high in sugar or white flour from misusing it.
Explore a new voluntary “nutrient density” labeling system or expanding existing nutrient content claims to cover positive attributes (e.g., “High in Magnesium” or a score reflecting vitamins per calorie).
Shifting the focus of labels from just calories and fat towards nutritional quality
Ease regulations around truthful, evidence-based health claims for foods and dietary programs.
Create a pathway for food-as-medicine claims – perhaps modeled on the existing “qualified health claim” system but expanded
Ensure overall strategy and regulatory posture supports the emerging ecosystem of food-as-medicine
Consider directing agencies like the Centers for Disease Control and Prevention (CDC) and the Agency for Healthcare Research and Quality (AHRQ) to incorporate metrics of preventive health success (e.g. rates of improvement in diet quality, physical activity levels, metabolic health indicators) into national health goals
Convene cross-agency initiatives with USDA to align agricultural subsidies and food assistance programs with nutrition outcome
Allow Medicare Advantage plans to offer food is medicine without regulatory scrutiny and even share savings with it’s members directly if it lowers the diabetes or obesity prevalence in its member population through nutrition and lifestyle interventions
Cover lifestyle medicine interventions for those with chronic disease and evaluate coverage for rising risk individuals before they progress to disease
Ensure that rules around wellness programs (like employer-sponsored health programs or HSAs/FSA spending) are flexible enough to include things like healthy meal services, exercise programs, continuous health monitoring devices, and stress reduction classes. Such expenses should be considered legitimate health investments
With a new framework that is aligned to support a new combined economy centered around human health not simply producing inexpensive food and treating people with disease. In the long term, rebuilding our food supply on principles of nutrient density and regenerative agriculture could reverse and prevent disease on a vast scale by ensuring that the default diet is genuinely health-promoting. This requires a partnership between the food industry and the healthcare industry and policy to support affordable nutrition and lifestyle medicine. And importantly, it does not require massive new government spending, but rather a realignment of existing regulations and incentives to focus on human health. Private sector innovation and consumer demand will do the rest.
The outcome will be a new economy that changes human health in daily life:
When you walk in the grocery store it is hard to make a bad nutrition decision.
The health benefit of food is clear to consumers
Everyone measures their A1c and with a lifestyle coach adapts to what works
Consumers easily understand the lifetime value of better food
Consumers understand how to incorporate food to replace pharmaceuticals
Consumers use food to reverse certain chronic disease, not treat it
Consumers understand the value of food over sickcare
Agriculture and the supply chain can capture the value of producing differentiated nutritional quality and taste over yield
We have an evidence-based understanding of nutrition equal to or better than our understanding of healthcare intervention
Food companies see their role in nutrition
Grocery becomes about nutrition, not shelf space
In summary, the “Food is Health” revolution is already underway, led by entrepreneurs, healthcare disruptors, and individuals taking charge of their well-being and focusing on restoring human health. To fully unlock this promising future, HHS must update its regulatory stance: shifting from a posture of cautious, siloed control toward one of facilitation and integration. By removing outdated barriers and encouraging innovation-friendly rules, the Department can unleash a wave of private-sector solutions that make Americans healthier at a fraction of the current cost while eradicating the chronic disease epidemic. Such regulatory realignment is squarely within the mandate of “ensuring lawful regulation and unleashing innovation.”
Thank you for considering these comments. We applaud HHS for taking on this initiative to examine and reduce regulatory impediments in healthcare. By embracing the deregulatory recommendations above, HHS can help accelerate the transition to a regulatory framework focused on human health and aligned with a “Food is Health” paradigm, that will benefit all Americans by improving quality of life. We are grateful for your leadership and would welcome any further dialogue as the Department advances these critical goals.
Sincerely,
Carter Williams & Ellen Brown
Food Is Health Revolution
Badass!